In this study, we used an economics research method to evaluate the cost-effectiveness of the GnRH-agonist long-protocol and the GnRH-antagonist protocol for IVF. We found that in the fresh embryo transplantation cycle, there was no significant difference in the ongoing pregnancy rate between the GnRH-agonist long-protocol and the GnRH-antagonist protocol, while the cost in the GnRH-antagonist protocol was lower, so GnRH-antagonist protocol has advantage according to the principle of cost-minimization analysis of pharmacoeconomics. When considering the cumulative ongoing pregnancy rate after each ovarian stimulation, the cumulative ongoing pregnancy rate and cost in the GnRH-agonist long-protocol were higher than the GnRH-antagonist protocol. Using the cost-effectiveness analysis method, it was found that the average cost of each ongoing pregnancy in the GnRH-agonist long-protocol was lower than the GnRH-antagonist protocol. Therefore, the GnRH-agonist long-protocol is more cost-effective.
Studies have shown that one of the primary reasons for dropout from infertility treatment is economic burdens . China’s medical system does not provide insurance coverage for infertility diagnosis and treatment. It can be an enormous economic burden to patients seeking ART. Therefore, no matter from the perspective of patients, or from the perspective of medical resource allocation, it is necessary to carry out economic analysis on IVF and consider the cost and effect of each step. Although GnRH-agonist long-protocols and GnRH-antagonist protocols have been widely used in IVF, there is still an ongoing debate about the results of the two protocols. Orvieto and Grow found the GnRH-agonist protocol has a superiority over the GnRH-antagonist protocol in live birth rate. Some studies also found no significant difference in the rates of live births or ongoing pregnancies between the two protocols. However, these studies are only from the perspective of clinical results, not from the perspective of economics. In our research, we hope to be able to focus more on evaluating the cost-effectiveness of both protocols, not just the clinical outcomes, which are just a link in the evaluation. After consulting the literature, we found that there have been little economic studies on the two different ovarian stimulation protocols used in IVF. Wei Pan et al. conducted a retrospective analysis of the cost-effectiveness of GnRH-a protocols, GnRH-ant protocols and GnRH-a ultra-long protocols. They used the live birth rate as one outcome of the study. However, it is difficult to calculate the cost throughout pregnancy. In order to ensure that the results are more reliable, we used the ongoing pregnancy rate as the end point of this economic study.
The cost of IVF treatment for infertility (the cost per ongoing pregnancy) in this study was higher than the average hospitalization cost for 30 diseases in 2018 according to the national bureau of statistics. IVF is a complex process involving ovarian stimulation, ovum retrieval, fertilization, embryo transfer and other processes. In addition to the cost of these processes, the total cycle costs of IVF should also include the transportation costs, lost wages and the cost of treating OHSS. However, it is difficult to accurately assess the transportation costs and lost wages and these indirect cost consisted a small percentage of the total costs, many studies did not include them in the total cycle cost analysis. But, from the perspective of patients, these costs are indirect medically, yet direct economically to patients, so they are also included in this study. OHSS is a serious complication of IVF, and the treatment is expensive, which directly affects the total cycle costs. Studies have shown that the incidence of OHSS in the GnRH-antagonist protocol is lower than that in the GnRH-agonist long-protocol. Accordingly, the cost of treating OHSS in the GnRH-antagonist protocol is lower, resulting in reduction in the total cycle cost. This may be one of the reasons why the cost in GnRH-antagonist protocol is lower than the GnRH-agonist long-protocol in the fresh embryo transfer cycle.
Economic analysis of IVF is still challenging, and there is no unified view on the result indicators of the analysis. Existing economic studies often used ongoing pregnancy, live birth rates or quality-adjusted life years (QALYs) as result of the study. However, it is worth considering that QALYs of both husband and wife or child is used when taking QALYs as a result of IVF. Toftager et al. found that quality of life and psychosocial and physical well-being of patients used the GnRH-antagonist protocol was better than that used the GnRH-agonist protocol. But these are hard to quantify in terms of costs. And it’s difficult to calculate the impact on families and society of obtaining a healthy baby by IVF. Considering the different incidence of related complications during pregnancy, the treatment costs and nursing costs vary greatly. Therefore, in this study, we used the cumulative ongoing pregnancy rate as the effect of the study.
There are many economic analysis methods, but among the existing studies on economics in ART, 84% are cost-effectiveness analysis and 48% are model-based studies
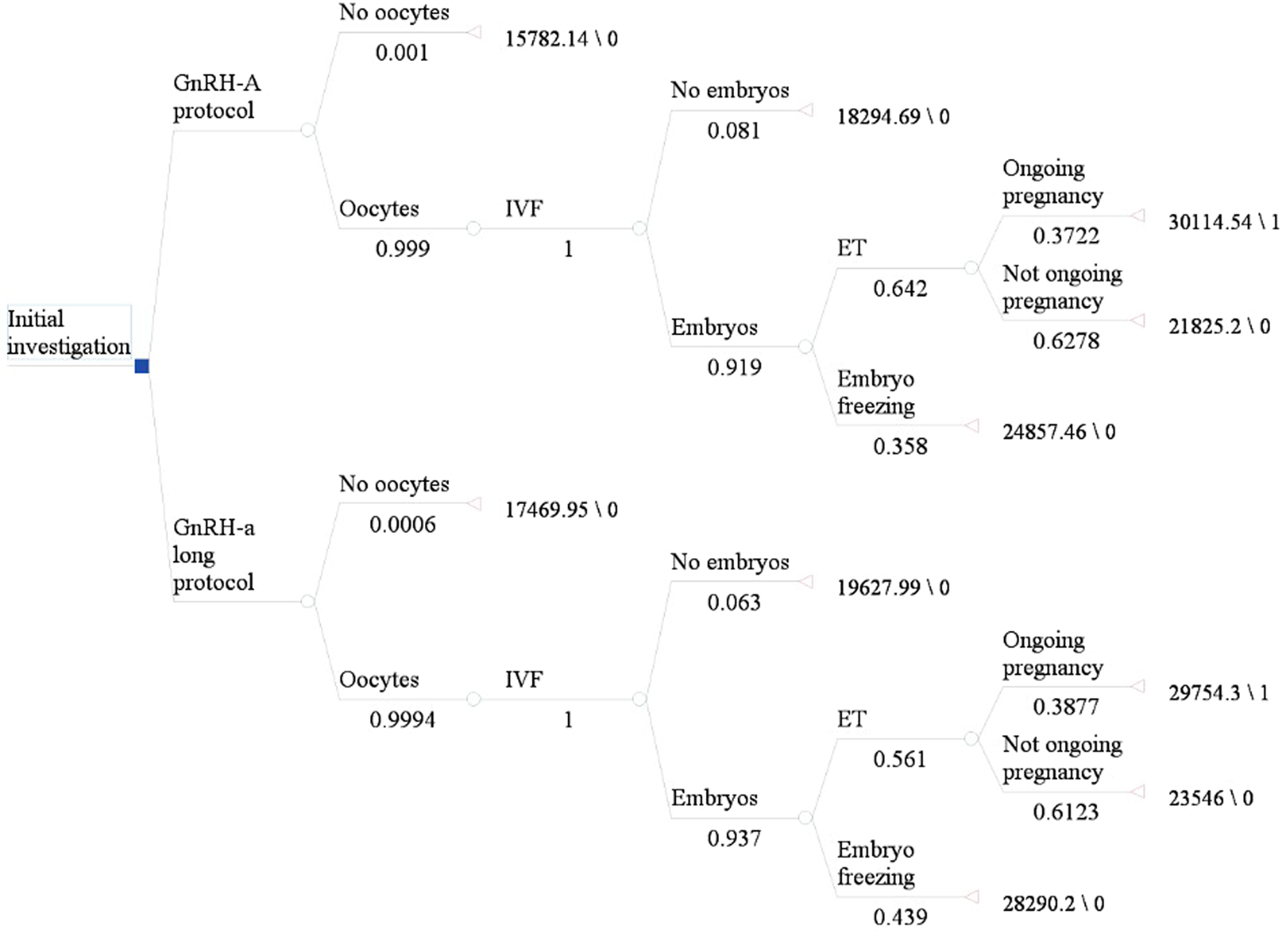
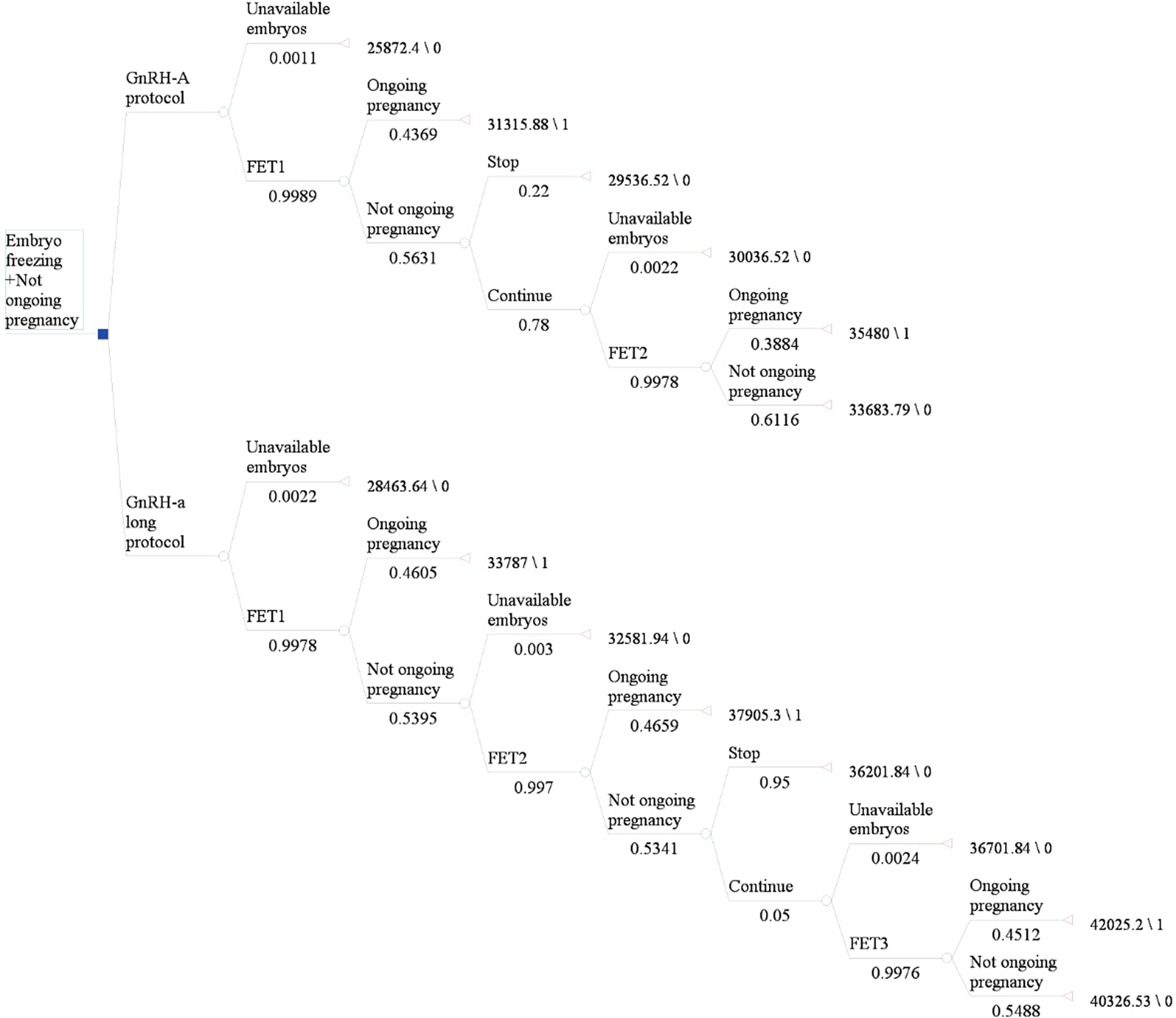
11. Economic model carried out before a trial is particularly useful in reducing unnecessary waste of research resources in evaluating techniques and interventions and improving the quality and efficiency of the research. In our study, we developed a decision-tree model to evaluate the cost-effectiveness of the GnRH-agonist long-protocol and GnRH-antagonist protocol. The relevant transfer probability in the model was calculated using the data of infertile patients in the reproductive center of our hospital. In addition, we have made some reasonable assumptions for analysis, as shown in Table 2.
This is a retrospective study on the data available from infertility diagnosis and treatment in our reproductive center. The relevant probability and costs in the model are calculated based on the data of our single center. These results may differ from those of other centers, but can provide some guidance for patients and clinicians. In the future, large samples, multi-center prospective randomized controlled trials are needed to more thoroughly explore more economical and effective treatment protocols.
In conclusion, if fresh embryo transfers are considered, the pregnancy outcomes between GnRH-agonist long protocols and GnRH-antagonist protocols are similar, but GnRH-antagonist protocols have lower cost. Therefore, in the fresh embryo transfer cycle, the GnRH-antagonist protocol has economic advantage and is worth recommending. However, GnRH-agonist long-protocol have higher success rates and higher costs when cumulative ongoing pregnancy rates are taken into account. The cost per ongoing pregnancy in the GnRH-agonist long-protocol cycles was lower than that in the GnRH-antagonist protocol cycles. Thus, cost-effectiveness analysis shows that the GnRH-agonist long-protocol is more cost-effective than the GnRH-antagonist protocol and may represent a cost-effective option from the perspective of patients. However, further large sample sizes and multi-center randomized controlled trials are needed.










.jpeg)


